Breaking Barriers in Cancer Care: Embracing Multilevel Strategies for a Healthier Tomorrow
- gilliangillies0
- Feb 17, 2024
- 8 min read
Updated: Mar 28, 2024
Navigating the Transition: Understanding the Shift
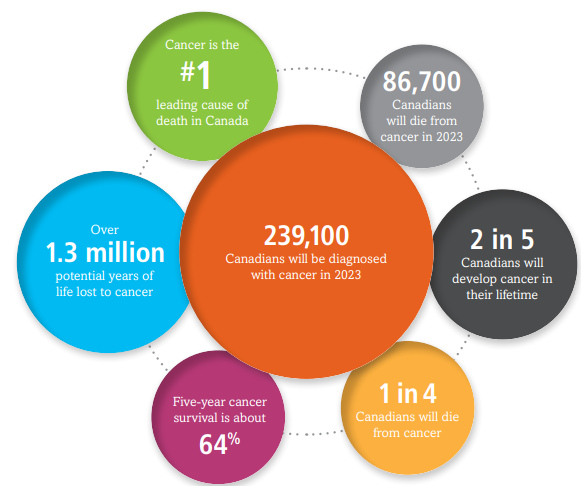
As a healthcare professional specializing in cancer care, each day I'm reminded of the intricate web that connects health outcomes to the broader determinants of health and the persistent challenges of health inequities. Since the 1950s, the nature of disease has changed considerably, and chronic diseases are now increasing worldwide (Huber, 2011). My home province of New Brunswick (N.B) has one of the highest rates of chronic health conditions in Canada, with 67.2% of the population reporting living with a chronic disease (NBHC, 2022). In my practice within cancer care, it's routine to encounter patients living not only with cancer as a disease but also with various chronic conditions such as hypertension, chronic obstructive pulmonary disease (COPD), diabetes, cardiovascular disease (CVD), and congestive heart failure (CHF) (Kone, 2021). In 2023, it was predicted that 45% of Canadians were expected to be diagnosed with cancer in their lifetime (Figure 1). It is evident how the intersection of cancer and chronic diseases imposes a substantial burden on healthcare systems (Canadian Cancer Society, 2023).
Figure 1 Lifetime probability of developing cancer (Canadian Cancer Society, 2023)

Even prior to the COVID-19 pandemic, the Canadian Cancer Society had already projected added pressures on cancer care services, predicting an increase of 79% in cancer cases by 2028–2032. COVID-19 has generated significant disruptions in oncology care provision that are likely to have lingering adverse effects across the cancer care trajectory for years to come (Chaput, 2021). These trends have also been observed globally. The United Nations convened in 2017 to tackle disparities in cancer care, highlighting the disproportionate impact on developing nations. It was emphasized that by 2030, more than two-thirds of cancer-related deaths will occur in these developing regions of the world (Video 1) (United Nations, 2017). Given the evolving nature of diseases, it's crucial to consistently evaluate the multilevel models of health within cancer care, emphasizing the etiologic component and biological dimensions (Lynch, 2013). Failure to do so may lead to less-than-ideal patient outcomes and impede progress in treatment development.
Video 1. Cancer Care Access (United Nations, 2017)
Cancer Care Continuum
Health-care delivery must occur in a multilevel system that includes, organizations, teams, and individuals (Taplin 2012). Multilevel models present an innovative alternative way for investigating health disparities and population health. Multilevel approaches and life course approaches may be the two most important paradigmatic shifts in population health sciences (Galea, 2015). Cancer care is a excellent example for considering the process of health-care delivery and multilevel systems because it spans the continuum of health-care issues from primary prevention through long-term survival and end-of life care.
But Not So Fast - Let's Understand Health Disparities
Even on the onset of a cancer diagnosis, health disparities emerge. Delays in the initiation of patients’ cancer treatment can worsen clinical outcomes, and more often affect vulnerable populations, including patients from underserved racial and ethnic groups, those with lower incomes, low-resources, and highly deprived neighborhoods. This highlights that the factors contributing to delays in cancer care are nuanced, multilevel, and often influenced not only by clinical factors, but social determinants of health (SDOH) (Frosch, 2023). Multilevel learning models incorporating SDOH have successfully estimated the likelihood of delays in starting cancer therapy, particularly on vulnerable populations (Taplin, 2012).
Socioeconomic factors are strong predictors of all-cause mortality and shortened life expectancy in many western countries (Albano, 2007). It is widely recognized that race and socioeconomic status includes mortality patterns and life expectancy (Albano, 2007). Literature shows a correlation between education level and health literacy to patient involvement in their own care (Heuser, 2019).
Educating and using “spheres of influence” as a concept can help the care teams and clinicians. Clinicians should recognize the importance of incorporating SDOH in their practices and embedding system-wide screenings, such as standardized questions like, “Have you been able to get everything you need to manage your health including groceries, medications, and transportation services?” (Karches, 2021). Exploring social support, especially emotional and informational, should be encouraged, as it has been shown to boost health and longevity. This support acts as a buffer during high-stress situations like cancer (Sauer, 2019).
In an interview in 2020, Dr. L. Pierce, the President of the American Society of Clinical Oncology (ASCO), emphasized the necessity of accounting both biological and socioeconomic disparities to comprehend the roots of inequality issues, highlighting the significance of SDOH in caring for cancer patients. The full interview is featured in the video below:
Video 2. Health inequities in Cancer Care (Breast Cancer Research Foundation, 2020)
Diving into a Multilevel Framework
Historically, multilevel approaches tend to focus on social and environmental hypotheses, and specifically when assessing cancer care, some models are limited in their ability to integrate biologic factors into a multilevel framework. I touched briefly on one study above (Frosch, 2023) that highlighted a multilevel approach to accurately determine which patients are at risk for oncology treatment delays in vulnerable populations, however this didn't fully include a biologic piece. One Multilevel framework to address the complex nature of cancer occurrence and outcomes is with a biologic multilevel model. Lynch (2013) proposed a "Multi-level Biologic and Social Integrative Construct" (MBASIC). Newer multilevel approaches like MBASIC have been developed to assess disease or cancer illness within hierarchical levels including the:
(1) Macroenvironment level (this would include health care policy, neighborhood, or family structure);
(2) Individual level (things like behaviors, carcinogenic exposures, socioeconomic factors, and psychologic responses); and
(3) Biologic level (focusing more on cellular biomarkers and genetics) (Lynch, 2013).
MBASIC is a model to integrate macroenvironment and individual factors with biology.
To address the complex nature of cancer etiology, multilevel approaches have been developed to assess the role of two or more etiologic agents within a structure. Multilevel conceptual frameworks are based on the premise that factors affecting disease act within and across levels (macro, individual or biologic) to collectively affect disease (Table 1) (Lynch 2013).
Table 1 : Hierarchical level definition : Macroenvironment, individual and Biologic (Lynch, 2013)

MBASIC is a multilevel framework that includes three main hierarchal levels that contribute to cancer etiology and levels of carcinogenesis (biologic factors). This is depicted visually in Figure 2 (Lynch, 2013). This multilevel model is placed in the context of interventions and implementation. This approach is positive because the framework allows researchers (from the fields of public health, health policy, prevention, behavioral sciences, sociology, epidemiology, biology, and clinical medicine) to test hypotheses of interest under a common conceptual framework to address the dynamic nature of cancer disease and genetic mutations. It also aids researchers in translating multilevel studies into clinical and public health strategies.

Figure 2 Multilevel Biologic and Social Integrative Construct (Lynch, 2013).
MBASIC framework is extremely beneficial for cancer outcomes. Lets use prostate cancer as an example. Prostate cancer is the most common cancer among Canadian men, and is the third leading cause of cancer-related death in Canadian men (Canadian Cancer Society, 2023).

Figure 3 Percentage of projected new cancer cases, by sex in Canada (Canadian Cancer Society, 2023)
Despite previous research, much remains unknown about the disease's origins and prognosis indicators. Current risk factors center on race (African American men facing a disproportionately higher risk), age, and family history. Diagnostic markers like Prostate-Specific Antigen (PSA) levels provide imperfect insights. The evolution of PSA screening, from cellular research in the 1980s has led to widespread screening. While PSA screening aims for early detection, its effectiveness in reducing mortality rates remains debated, with concerns about over diagnosis and undertreatment. Historically, the FDA has approved the biopsy of PSA values above 4.0 mg/mL for cancer detection (Atan, 2013). However, some individuals with PSA levels below 4.0 ng/mL have prostate cancer and many with higher PSA levels between 4.0 and 10.0 ng/mL do not have prostate cancer (Thompson, 2004). Ongoing research seeks to refine screening protocols, acknowledging individual risk factors and socioeconomic disparities. The PSA screening process (spanning from cellular origins to clinical implementation) underscores the intricate interplay between individual biomarkers and societal influences on screening guidelines, healthcare systems, and cancer outcome disparities (Lynch, 2013). Multilevel approaches, like the MBASIC framework, offer a much more promising avenue for optimizing prostate cancer screening and treatment strategies by integrating biological, individual, and environmental factors. This holistic approach emphasizes collaboration across disciplines to address the complexities of prostate cancer disparities and improve patient outcomes at a cellular level.
Conclusion
Multilevel approaches provide advantages over conventional models (Evans et al 2018). Multilevel approaches in oncology services are essential for addressing the increasing complexity of cancer care. Additionally, we need to enhance the overall effectiveness of safe, equitable, and accessible patient care while translating research into best practices. With the percentage of chronic diseases increasing worldwide, adopting a multilevel framework is paramount for success in alleviating the burden. Cancer is not a single event with a certain end, it is an enduring condition characterized by ongoing uncertainly (Miedema, 2013). Multilevel approaches must not only focus on social and environmental hypotheses but also on integrating biologic factors into a multilevel framework. I strongly feel if we want to improve healthcare performance and enhance accessibility for vulnerable oncology patients, incorporating the biological component is instrumental.
References:
Albano, J. D., Ward, E., Jemal, A., Anderson, R., Cokkinides, V. E., Murray, T., Henley, J., Liff, J., & Thun, M. J. (2007). Cancer Mortality in the United States by Education Level and Race. JNCI: Journal of the National Cancer Institute, 99(18), 1384–1394. https://doi.org/10.1093/jnci/djm127
American Cancer Society (2019, January 14). Managing Cancer as Chronic Disease Illness. Retrieved March 2, 2024, from https://www.cancer.org/cancer/survivorship/long-term-health-concerns/cancer-as-a-chronic-illness.html
Atan, A., & Güzel, Ö. (2013). How should prostate specific antigen be interpreted?. Turkish journal of urology, 39(3), 188–193. https://doi.org/10.5152/tud.2013.038
Breast Cancer Research Foundation. (2020, August 21). Tackling Health Inequities in Cancer Care: An Interview with ASCO President Dr. Lori Pierce [Video]. Breast Cancer Research Foundation. https://www.youtube.com/watch?v=WWGKsw_lEFk&t=6s
Canadian Cancer Society (2023, November 1). Prostate cancer statistics. Retrieved February 24, 2024, from https://cancer.ca/en/cancer-information/cancer-types/prostate/statistics
Chaput G, Lilly E. Oncology Care Provision: Planning for Today, Tomorrow, and Years to Come. Current Oncology. 2021; 28(6):4774-4775. https://doi.org/10.3390/curroncol28060403
Evans, C. R., Williams, D. R., Onnela, J.-P., & Subramanian, S. V. (2018). A multilevel approach to modeling health inequalities at the intersection of multiple social identities. Social Science & Medicine, 203, 64–73. https://doi.org/10.1016/j.socscimed.2017.11.011
Frosch, Z. A. K., Hasler, J., Handorf, E., DuBois, T., Bleicher, R. J., Edelman, M. J., Geynisman, D. M., Hall, M. J., Fang, C. Y., & Lynch, S. M. (2023). Development of a Multilevel Model to Identify Patients at Risk for Delay in Starting Cancer Treatment. JAMA network open, 6(8), e2328712. https://doi.org/10.1001/jamanetworkopen.2023.28712
Galea, S. Boston University School of Public Health (2015, May 31). The Determinants of Health Across the Life Course and Across Levels of Influence. Retrieved February 10, 2024, from https://www.bu.edu/sph/news/articles/2015/the-determination-of-health-across-the-life-course-and-across-levels-of-influence-2/
Huber M, Knottnerus J A, Green L, Horst H v d, Jadad A R, Kromhout D et al. How should we define health? BMJ 2011; 343 :d4163 doi:10.1136/bmj.d4163
Karches, K., DeCamp, M., George, M., Prochaska, M., Saunders, M., Thorsteinsdottir, B., & Dzeng, E. (2021). Spheres of Influence and Strategic Advocacy for Equity in Medicine. Journal of general internal medicine, 36(11), 3537–3540. https://doi.org/10.1007/s11606-021-06893-4
Koné, A. P., & Scharf, D. (2021). Prevalence of multimorbidity in adults with cancer, and associated health service utilization in Ontario, Canada: a population-based retrospective cohort study. BMC Cancer, 21(1). https://doi.org/10.1186/s12885-021-08102-1
Lynch, S.M. and Rebbeck, T.R. (2013). Bridging the Gap between Biologic, Individual, and Macroenvironmental Factors in Cancer: A Multilevel Approach. Cancer Epidemiol Biomarkers Prev 1. 22 (4): 485–495. https://doi.org/10.1158/1055-9965.EPI-13-0010
Mahumud, R. A., Alam, K., Dunn, J., & Gow, J. (2020). The burden of chronic diseases among Australian cancer patients: Evidence from a longitudinal exploration, 2007-2017. PLOS ONE, 15(2), e0228744. https://doi.org/10.1371/journal.pone.0228744
Miedema, B., Easley J, Robinson LM. Do current cancer follow-up care practices meet the needs of young adult cancer survivors in Canada? A qualitative inquiry. Curr Oncol. 2013 Feb;20(1):14-22. doi: 10.3747/co.20.1207. PMID: 23443642; PMCID: PMC3557327.
New Brunswick Health Council (2022). Primary Care Survey. Retrieved February 16, 2024, from Needs of New Brunswickers. (2022). Nbhc.ca. https://nbhc.ca/table/needs-new-brunswickers?cuts=NB%2CNBZ1%2CNBZ2%2CNBZ3%2CNBZ4%2CNBZ5%2CNBZ6%2CNBZ7&gid=8207&sid=5284&tid=5284
Sauer, C., Weis, J., Faller, H., Junne, F., Hönig, K., Bergelt, C., Hornemann, B., Stein, B., Teufel, M., Goerling, U., Erim, Y., Geiser, F., Niecke, A., Senf, B., Weber, D., & Maatouk, I. (2019). Impact of social support on psychosocial symptoms and quality of life in cancer patients: results of a multilevel model approach from a longitudinal multicenter study. Acta oncologica (Stockholm, Sweden), 58(9), 1298–1306. https://doi.org/10.1080/0284186X.2019.1631471
Statistics Canada. (2023). Profile table, Census Profile, 2021 Census of Population - Fredericton (Census metropolitan area), New Brunswick (statcan.gc.ca)
Taplin, S. H., Anhang Price, R., Edwards, H. M., Foster, M. K., Breslau, E. S., Chollette, V., Prabhu Das, I., Clauser, S. B., Fennell, M. L., & Zapka, J. (2012). Introduction: Understanding and Influencing multilevel Factors Across the Cancer Care Continuum. JNCI Monographs, 2012(44), 2–10. https://doi.org/10.1093/jncimonographs/lgs008
Thompson, I. M., Pauler, D. K., Goodman, P. J., Tangen, C. M., Lucia, M. S., Parnes, H. L., Minasian, L. M., Ford, L. G., Lippman, S. M., Crawford, E. D., Crowley, J. J., & Coltman, C. A., Jr (2004). Prevalence of prostate cancer among men with a prostate-specific antigen level < or =4.0 ng per milliliter. The New England journal of medicine, 350(22), 2239–2246. https://doi.org/10.1056/NEJMoa031918



Comments