Threads of Insight: Exploring the Interconnected World of Cancer Care
- gilliangillies0
- Apr 2, 2024
- 9 min read

My journey over the last few months throughout my Master’s in Health Studies has been humbling and enlightening. As I reflect through this educational journey, I find myself applying newfound knowledge to my role in the oncology field and within cancer care. The diverse perspectives of my peers and classmates who have focused on different health specialties have enriched my understanding in ways I hadn't anticipated. In this week's blog post, I aim to weave together these varied threads of learning, reflecting on their interconnectedness within the realm of cancer care, while also drawing from my professional practice as Director of Oncology and Ambulatory Care.
Cancer, as a disease, it affects everyone, regardless of demographic or social status. Yet, certain groups experience a disproportionate burden of cancer compared to others. Who are these groups? What does our healthcare system in Canada have in place to support them? Despite progress, access to cancer care remains a challenge for some. As we look to the future, what opportunities and obstacles lie ahead? These are questions that demand exploration and dialogue and I am grateful for having the opportunity to have explored them.
Throughout my last blog post for the course, I’ll illustrate key points and insights. I hope to foster a deeper understanding of the complexities in cancer care and inspire meaningful discussions about its future direction with my colleagues and patients.
A quick look back to the past
After World War II, acute disease was highly recognized, and now the nature of disease changed considerably. Chronic disease is now increasing worldwide (Huber, 2011). Last year, in 2023, it was predicted that 239,100 Canadians would be diagnosed with cancer, and 86,700 Canadians were expected to die from the disease. Cancer has also been noted as the leading cause of death in Canada (Canadian Cancer Society, 2023). Notably, certain cancer types, including ovarian cancer, chronic leukemias, some lymphomas, and metastatic breast or prostate cancer, can manifest as chronic illnesses (American Cancer Society, 2019). In my practice within cancer care, it's routine to encounter patients dealing not only with cancer but also with various chronic conditions. Surprisingly, research indicates that approximately 75% of individuals diagnosed with cancer have at least one other chronic health condition (Kone, 2021). Managing multiple chronic diseases not only increases the complexity of care but also heightens the risk of adverse outcomes (Mahamud, 2020). I’ll dive deeper in the complexities of chronic disease shortly.
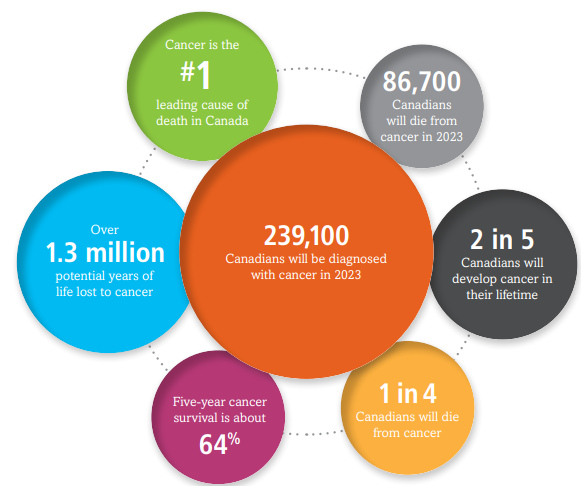
(Canadian Cancer Society, Canadian Cancer Statistics 2023)
Gaps in the Canadian Health Care System
At the start of my studies, my peers and I explored Canada's universal health care system. Particularly focusing on the situation in New Brunswick, there are significant gaps in access to primary health care (PHC) and mental health support for those experiencing cancer. In New Brunswick, 15% of citizens don’t have a primary care provider, and only 50.8% of New Brunswickers could get an appointment with their family doctor within five days in 2020. However, this percentage has declined to 34.1% in 2022, consistently across the province. Citizens in Northern New Brunswick experienced even worse timely access, with only 17% reporting being able to see their primary care provider within that timeframe (NBHC, 2022). Limited access to healthcare services, including screenings, early detection programs, and diagnostic tools, can impede timely cancer diagnosis and treatment initiation (Mahmud, 2020). This is problematic.
The current Canada Health Act (CHA) is not adequately addressing these issues, indicating a need for modernization and greater accountability for equal and equitable access to essential health services for all Canadians (Flood, 2017). These issues are exacerbated for those with chronic disease diagnoses, marginalized populations, or those affected by health inequalities.
Marginalized Groups
If the oncology patient is identified as belonging to a marginalized group, such as LGBTQ+ individuals, persons with disabilities, ethnic and racial minorities, immigrants, newcomers, or the elderly, the challenges in navigating cancer care become exacerbated. When examining racial disparities alone, differences in cancer outcomes can be attributed to variations in tumor biology, treatment efficacy, and the failure to provide optimal cancer care (Esnaola, 2012). Analyzing the determinants of race, researchers note that African American women have a higher likelihood of extremely dense breasts compared to other racial groups. Moreover, African American women are more likely to be diagnosed with metastatic breast cancer and have a higher mortality rate from breast cancer compared to non-Hispanic white women (Moore, 2020). To address these inequities and differences, we must take action here in New Brunswick by implementing recommendations from the Systemic Racism Commissioner’s Final Report. This report serves as an important reminder of the challenges faced by marginalized groups, urging us to work towards building a more inclusive and equitable society (Varma, 2022).
(CBS Miami, 2021)
Health Determinants
Adding another layer, I've realized throughout the course the true nature and complexity of health determinants and inequalities, on a global level and in Canada. I knew New Brunswick didn’t fare as well compared to other provinces, but I had no idea how much we are struggling in some areas of health, addressing these disparities, particularly in managing chronic disease. I was able to compare these differences with my classmates in Ontario and British Columbia. It's evident that social, economic, genetics, and education levels play a significant role in shaping health outcomes, particularly for marginalized populations. Socioeconomic factors are strong predictors of all-cause mortality and shortened life expectancy in many Western countries (Albano, 2007). It is widely recognized that race and socioeconomic status influence mortality patterns and life expectancy (Albano, 2007). Literature shows a correlation between education level and health literacy in patient involvement in their own care (Heuser, 2019).
Care providers should recognize the importance of incorporating determinants of health into their practices and embedding system-wide screenings (Karches, 2021). Exploring social support, especially emotional and informational, should be encouraged, as it has been shown to boost health and longevity (Sauer, 2019). Clinicians have to explore both biological (genetic factors) and socioeconomic disparities to comprehend the roots of inequality issues. It’s crucial to prioritize collaborative efforts and translate evidence-based research into action to address health disparities and ensure equal opportunities for health worldwide.
Chronic Disease
I want to take a moment to delve deeper into the complexity of the relationships between cancer and chronic diseases, which became very evident during my research studies and learning activities in my course. The prevalence of chronic conditions among cancer patients is complex, and managing multiple health issues simultaneously with cancer treatment increases the risk of adverse outcomes (Renzi, 2019). Recognizing the primary determinants influencing both cancer and chronic diseases, such as lifestyle choices, socioeconomic factors, and access to healthcare, highlights the importance of integrated, coordinated care pathways in optimizing patient outcomes. Moving forward, leveraging multidisciplinary team approaches and prioritizing coordinated management of chronic conditions are essential strategies in addressing the unique needs of cancer patients with chronic diseases (Phillips, 2010).
Chronic diseases can be influenced by lifestyle choices, genetics, and race, all of which play a crucial role in shaping cancer incidence, progression, and treatment outcomes. Unhealthy lifestyle choices and habits such as smoking, excessive alcohol consumption, poor diet, lack of physical activity, and obesity are well-established risk factors for various types of cancer (Jiang, 2021; Mahmud, 2020).
There are many interconnecting chronic conditions that coexist within cancer care. In my practice within cancer care, it's routine to encounter patients living not only with cancer but also with various chronic conditions such as hypertension, chronic obstructive pulmonary disease (COPD), diabetes, cardiovascular disease (CVD), and congestive heart failure (CHF) (Kone, 2021).
Surprisingly, research indicates that approximately 75% of individuals diagnosed with cancer have at least one other chronic health condition (Kone, 2021). Managing multiple chronic diseases not only escalates the complexity of care but also heightens the risk of adverse outcomes (Mahmud, 2020). My home province of New Brunswick (N.B) has one of the highest rates of chronic health conditions in Canada, with 67.2% of the population reporting living with a chronic disease (NBHC, 2022). Unfortunately, when trying to balance the treatment and management of cancer, chronic conditions are often managed separately or not at all; however, coordinated management could enhance patient outcomes (Kone, 2021).
Multilevel framework
An excellent solution to these challenges is a multilevel framework approach. Cancer care can be complex, and there is great importance in addressing health disparities through multilevel approaches. By incorporating multiple models of health and disease, we can better comprehend the intricate interplay between biological, environmental, and determinants of health, thus improving our ability to develop effective interventions and strategies (Lynch, 2013). Moving forward, it's crucial to integrate multilevel frameworks to improve healthcare performance and accessibility for vulnerable oncology patients and other health specialties. Early diagnosis remains paramount in improving cancer outcomes (Renzi, 2019), especially given the number of new diagnoses. In general, it is expected that cancer incidence rates for 2023 will be highest in eastern and central Canada (Canadian Cancer Statistics, 2023).
Future Health
As I have just summarized, Canadians and people across the world face many health inequalities, but the future of healthcare and research has transformative advancements that are shaping cancer care and health outcomes like never seen before. Emerging trends such as Artificial Intelligence (AI), genomic medicine, robotic surgery, and other innovative treatment therapies give me great optimism as I am convinced these tools will improve patient outcomes. These advancements and technologies offer great opportunities for early detection, personalized treatment, and enhanced effectiveness in cancer care (Majumder, 2021). As I reflect on these innovations, I'm inspired by the collaborative efforts of researchers and healthcare professionals worldwide.
Conclusion
I am incredibly grateful to have gained new insights into the complexities of cancer care and its connections with chronic diseases and inequities. Reflecting on the gaps within the healthcare system (particularly in addressing marginalized groups and recognizing the critical role of social determinants of health) I must emphasize in my final post the urgent need for equity and inclusivity in our healthcare approaches. We must start by adopting a multilevel framework approach alongside holistic strategies to enhance healthcare accessibility and outcomes for vulnerable populations. Looking ahead, I'm optimistic about transformative advancements and technologies in healthcare, such as AI and genomic medicine. I am confident that these innovations will address the growing need for early detection and personalized treatment in cancer care. It's been a pleasure sharing this journey with you all. Thanks!

References
Albano, J. D., Ward, E., Jemal, A., Anderson, R., Cokkinides, V. E., Murray, T., Henley, J., Liff, J., & Thun, M. J. (2007). Cancer Mortality in the United States by Education Level and Race. JNCI: Journal of the National Cancer Institute, 99(18), 1384-1394. https://doi.org/10.1093/jnci/djm127
Canadian Cancer Society (n.d.). Cancer as a chronic disease. Canadian Cancer Society. Retrieved March 4, 2024. https://cancer.ca/en/living-with-cancer/life-after-treatment/cancer-as-a-chronic-disease
Canadian Cancer Society (2023, November 1). Canadian Cancer Statistics. Retrieved March 4, 2024, from 2023_pdf_en.pdf (cancer.ca).
Esnaola, N. F., & Ford, M. E. (2012). Racial differences and disparities in cancer care and outcomes: Where’s the rub? Surgical oncology clinics of North America. 21(3), 417-437. https://doi.org/10.1016/j.soc.2012.03.012
Flood, C. M., & Thomas, B. (2017, February 27). Modernizing the Canada Health Act. Ottawa University Faculty of Law. Retrieved March 27, 2024, from https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2907029
Heuser, C., Diekmann, A., Kowalski, C., Enders, A., Conrad, R., Pfaff, H., Ansmann, L., & Ernstmann, N. (2019). Health literacy and patient participation in multidisciplinary tumor conferences in breast cancer care: a multilevel modeling approach. BMC cancer, 19(1), 330. https://doi.org/10.1186/s12885-019-5546-z
Huber M, Knottnerus J A, Green L, Horst H v d, Jadad A R, Kromhout D et al. How should we define health? BMJ 2011; 343 :d4163 doi:10.1136/bmj.d4163
Jiang, C., Deng, L., Karr, M. A., Wen, Y., Wang, Q., Perimbeti, S., Shapiro, C. L., & Han, X. (2021). Chronic comorbid conditions among adult cancer survivors in the United States: Results from the National Health Interview Survey, 2002‐2018. Cancer. https://doi.org/10.1002/cncr.33981
Koné, A. P., & Scharf, D. (2021). Prevalence of multimorbidity in adults with cancer, and associated health service utilization in Ontario, Canada: a population-based retrospective cohort study. BMC Cancer, 21(1). https://doi.org/10.1186/s12885-021-08102-1
Lynch, S.M. and Rebbeck, T.R. (2013) Bridging the Gap between Biologic, Individual, and Macroenvironmental Factors in Cancer: A Multilevel Approach. Cancer Epidemiol Biomarkers Prev. https://doi.org/10.1158/1055-9965.EPI-13-0010
Mahumud, R. A., Alam, K., Dunn, J., & Gow, J. (2020). The burden of chronic diseases among Australian cancer patients: Evidence from a longitudinal exploration, 2007-2017. PLOS ONE, 15(2), e0228744. https://doi.org/10.1371/journal.pone.0228744
Majumder, A., & Sen, D. (2021). Artificial intelligence in cancer diagnostics and therapy: current perspectives. Indian Journal of Cancer. 58(4), 481–492. https://doi.org/10.4103/ijc.IJC_399_20
Moore, J.X., Han, Y., Appleton, C., Colditz, G., and Toriola, A.T. (2020). Determinants of Mammographic Breast Density by Race Among a Large Screening Population. JNCI Cancer Spectrum. 4(2). doi: 10.1093/jncics/pkaa010
New Brunswick Health Council (2022). Primary Care Survey. Retrieved February 16, 2024, from Needs of New Brunswickers. (2022). Nbhc.ca. https://nbhc.ca/table/needs-new-brunswickers?cuts=NB%2CNBZ1%2CNBZ2%2CNBZ3%2CNBZ4%2CNBZ5%2CNBZ6%2CNBZ7&gid=8207&sid=5284&tid=5284
Phillips, J. L., & Currow, D. C. (2010). Cancer as a chronic disease. Collegian, 17(2), 47–50. https://doi.org/10.1016/j.colegn.2010.04.007
Renzi, C., Kaushal, A., Emery, J. (2019). Comorbid chronic diseases and cancer diagnosis: disease-specific effects and underlying mechanisms. Nat Rev Clin Oncol 16, 746–761. https://doi.org/10.1038/s41571-019-0249-6
[YouTube]. (2021, October 27). Research Shows Significant Disparities For Black Women In Breast Cancer Detection & Treatment [Video]. CBS Miami. https://www.youtube.com/watch?v=rOc1BCCTSF8
Varma, M. (2022, December 1). Systemic Racism Commissioner’s Final Report 2022. Government of New Brunswick. Retrieved March 6, 2024, from https://www2.gnb.ca/content/dam/gnb/Corporate/Promo/systemicracism-racismesystemique/SystemicRacismCommissionerFinalReport.pdf



Comments